Author

Ann Harrington
Senior Writer
The scarcity of doctors in small communities is a national phenomenon that is particularly pronounced in sparsely populated North Dakota. It’s a matter of uneven geographic distribution: Although the number of physicians practicing in the state is only slightly below the national average, they are concentrated in population centers, leaving many rural areas underserved (see chart).
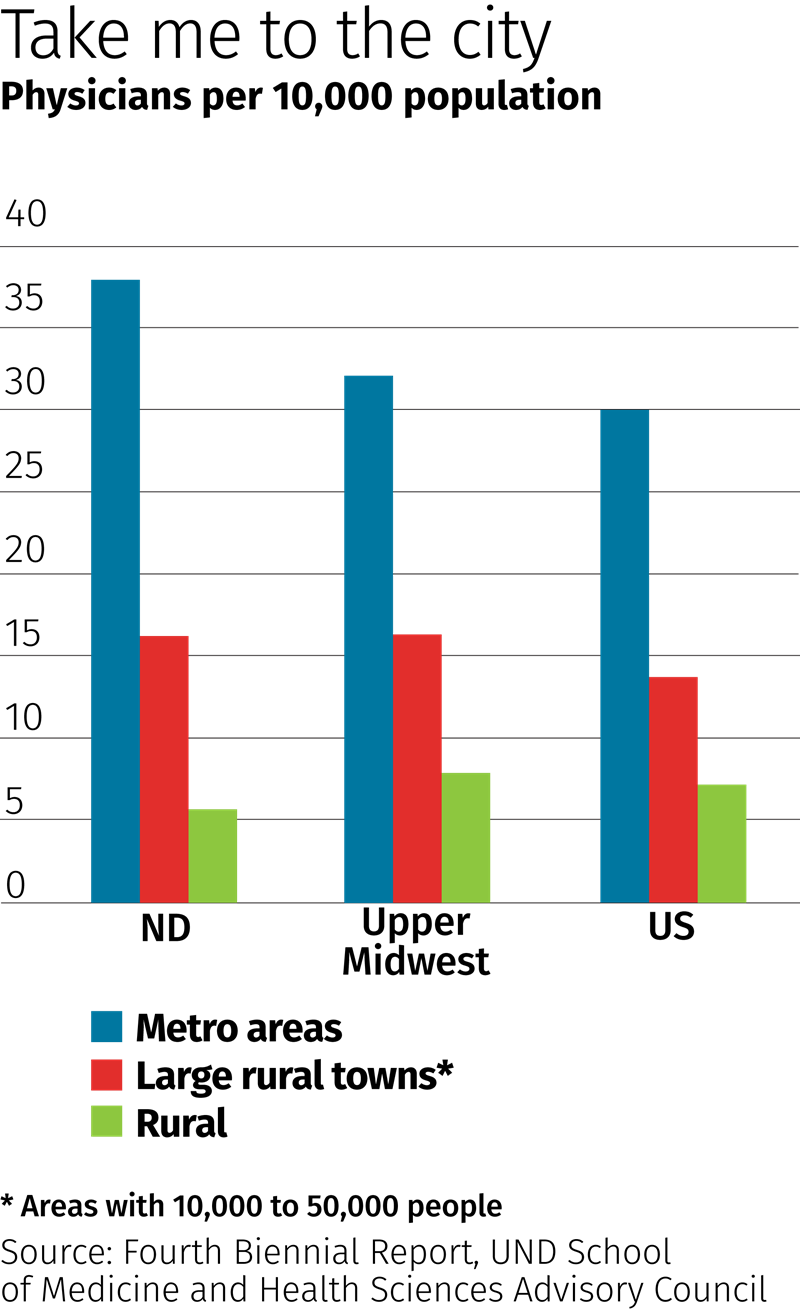
Rural areas of the state have about five times as many people per physician as metro areas such as Fargo and Bismarck, according to a recent report by the University of North Dakota. Thirteen counties have no practicing doctors at all.
North Dakota has taken steps to address this maldistribution of physicians and other health workforce challenges. Six years ago, the state put together a comprehensive plan to train more doctors and other health care providers and encourage them to practice in the state, particularly in rural areas.
Gary Hart is director of the Center for Rural Health at UND’s School of Medicine and Health Sciences and an expert on health workforce issues. He helped craft and implement the state Healthcare Workforce Initiative as a member of the school’s Advisory Council.
Hart spoke to the fedgazette about the roots of the doctor shortage in rural North Dakota and efforts to find solutions. The conversation has been edited for length and clarity.
fedgazette: Why are North Dakota’s physicians so concentrated in metro areas? Does the state’s geography play a part?
Hart: The geography has a great deal to do with it. The state has between 700,000 and 800,000 people, and about half the population lives in four cities—Fargo, Grand Forks, Bismarck and Minot.
Another factor is that most of the nation’s medical schools are in large cities. Take Boston, for instance. It’s a huge center of medical residents and a great system. But if you pick somebody out of North Dakota and send them to one of those medical schools, and they get married there, and enjoy the amenities of a big city, they are less likely to want to come back and practice in a small town.
For medical specialists, the main reason is economic: If you’re a neurosurgeon, you need a very large population to produce enough cases to support yourself. But if you’re a family physician, you need only 1,500 or 2,000 people to support yourself.
fedgazette: What are the consequences of fewer physicians per capita in rural areas? Does this scarcity translate into lower-quality care?
Hart: It depends. You have to be very careful how you define quality. Is there any reason to believe that rural physicians, individually, don’t practice medicine as well as urban physicians? The answer to that is no. They go to the same medical schools; there’s no reason to believe the quality of the trained professional is any different. What’s different are their backup systems, their facilities, the hospitals and their access to consults.
If there’s really a shortage of doctors in a town, the doctor may well be seeing a lot more patients, but doesn’t see them for as long. The alternative is the doctor saying, ‘I’m going to see fewer patients,’ in which case, half the people in town have to drive two hours to see a family physician for a cold. Then people are less likely to see their providers when they should. If you’re elderly and not feeling well, there’s a great cost to those long drives.
fedgazette: Rural populations tend to be older, and they’re aging faster than the U.S. population as a whole. What are the implications for physician supply and demand?
Hart: It means that when you’re trying to figure out how many physicians you need, you have to consider the fact that older populations require more of everything, especially physicians. I’ll give you an example. If you had a town filled with 14-year-old boys, they would average less than one primary-care visit a year. If there were only 85-year-old men in the town, they would average over a dozen visits a year—just primary care, not to mention specialists and hospitalizations. So, there is a big difference in demand, depending on the demographics.
fedgazette: Speaking of aging, almost half of the primary care doctors in rural North Dakota are 55 or older. That must raise concerns about the supply of doctors 10 or 20 years from now.
Hart: Well, of course, when you’re figuring out how many doctors you need, you figure it out into the future. You have to estimate how many retirements you’ll have and how many people will migrate in and out of your state. It costs a lot of money to produce a physician, so you don’t want to overproduce. On the other hand, the penalty for underproducing is sickness, pain and dying.
fedgazette: How do recent changes in federal immigration policy affect the role of foreign physicians in providing care in rural areas?
Hart: Some of this is so new that it’s hard to know the impact yet. International medical graduates (IMGs) represent just over a quarter of all physicians practicing in the state, slightly higher than the national average. They tend to work in hospitals more than in doctor’s offices, so they’re less likely to be in smaller towns. But we have a bunch of IMGs doing residencies here who are providing care to thousands of North Dakotans over three or four years. The leading suppliers of IMGs in the state are India, the Philippines and Pakistan. If this country appears to be an unstable environment for IMGs, I suspect fewer will choose to come here. And we’d have to make up the difference by training our own, which is expensive.
fedgazette: Telemedicine is seen as a possible solution to a tight supply of rural doctors. Is this technology helping to close the distances between practitioners and patients?
Hart: A lot of research has shown that providing psychological or psychiatric services via telemedicine to rural areas can be quite effective, especially for younger people who are more comfortable with the technology. It’s also being used in emergency situations, to give support to local docs. So telemedicine has shown great promise in certain circumstances, and it’s spreading across the country. One big obstacle to telemedicine was that, until recently, it wasn’t reimbursed well at all, if at all, in lots of places. Medicare and Medicaid have now made that easier, and third-party health insurers tend to follow their leads.
fedgazette: I can see that neither telemedicine nor importing doctors from abroad is likely to make up for a lack of primary-care providers in rural areas. What are UND and other stakeholders in North Dakota health care doing to train more doctors and health care workers, and to keep them around after graduation?
Hart: In 2011, the School of Medicine and its advisory committee looked at the dire forecast of health care workers not being able to keep up with population growth in the state and decided we need to grow more of our own. So the state Legislature increased the annual number of residency slots by 17, almost all in primary care, and expanded the size of the medical school class by 16. The legislation also provided funding to train more health science majors—physical therapists, occupational therapists, medical lab professionals, physician assistants.
fedgazette: I understand North Dakota has the lowest number of residency slots per med student in the country.
Hart: That’s one of the reasons for adding slots. An important thing that determines where doctors practice is where they do their residency. But adding slots costs the state a lot of money, because the federal government only pays for so many residency spots.
Another big determinant of where doctors end up is the location of their medical school and where they grew up. If you want more rural doctors, one of the things you can do is make a rural background a priority for acceptance into medical school and give extra points for it when you’re evaluating the students.
fedgazette: Nationwide, what initiatives have had the most success in increasing the number of doctors practicing in small communities?
Hart: There’s a whole series of initiatives in places like UND and the University of Minnesota to have medical students and residents spend more time in rural areas. Take residencies, for example; almost none of the residency training in the country takes place in rural areas.
If you look at what a family doctor in a rural area does compared to a family physician in urban areas, the rural doctors see far more diagnoses, they do far more procedures and their practice is much broader. You’re going to have to be better at more things. But you’re also probably going to be more a part of the community, which can be very rewarding.
Working at a hospital in an urban area, you’ve got all the backup in the world—if you’re not sure about something, you can get quick referrals or walk down the hall and get another opinion. But when you’re out in rural areas, you’re going to have to do more and be responsible for more. You’ve got to get residents comfortable with that and help them experience the benefits of working in a smaller community. If they’re not comfortable, they’re not going to go to rural areas, or if they go, they’re not going to stay.
fedgazette: Thank you, Gary.


