Author



The waiting list for an apartment just got shorter at Elm Crest Manor & Assisted Living in New Salem, N.D. In July, Elm Crest was planning to open nine assisted living apartments for elderly people who can no longer stay in their homes but don’t require around-the-clock nursing care.
Founded as a nursing home by the Peace Church of New Salem in the 1960s, Elm Crest first branched out into assisted living in 2001, building 10 small apartments adjacent to the nursing home. Over the past decade, demand for the apartments was high in the small town 30 miles west of Bismarck; seniors were typically waiting three to four years for an apartment to open up.
The expansion helps to meet that pent-up demand, said Elm Crest Administrator Janessa Vogel. The new apartments were already spoken for by seniors—many of them women in their 80s living alone—seeking the security and social support that assisted living offers.
“Obviously, there’s that need out there; I’ll easily fill them all up,” Vogel said. “These apartments are giving the community more choices. There isn’t a need in the area for more nursing home beds because we’re so close to Bismarck-Mandan, and a lot of surrounding communities have nursing homes. But there are not a lot of communities in our area that have assisted living.”
Assisted living is an expanding segment of the Ninth District’s long-term care industry, catering to elderly and disabled people who want to maintain an independent lifestyle while having ready access to medical care and help with daily activities. Assisted living options range from small facilities such as Elm Crest in rural communities and city neighborhoods to large urban complexes with swimming pools, wellness centers and other amenities. Some assisted living providers cater to residents with dementia and other severe disabilities.
Across the country and in many parts of the district, assisted living is displacing nursing homes, for decades the model of care for those who cannot safely live on their own. In Minnesota and Wisconsin, assisted living facilities have proliferated, while nursing homes have declined.
The shift is “part of our picture of aging that we want to be independent as long as possible, and if we can’t be independent, we want the setting where we live to be as normal as possible, a setting that we associate with other aspects of our life,” said Gayle Kvenvold, president of LeadingAge Minnesota, an umbrella group for organizations serving Minnesota seniors.
Assisted living is also attractive financially; on average, the cost of room and board in an assisted living facility is roughly half that of nursing home care. However, costs still are a barrier for seniors and the disabled with low or moderate incomes; some assisted living providers turn away prospective tenants on Medicaid because of low government reimbursement rates.
Like nursing homes, assisted living facilities have struggled to hire and hold onto workers. “That is challenge number one in many respects for us, today,” Kvenvold said. An economy on the upswing after the Great Recession has made matters worse, increasing job vacancies and turnover at assisted living facilities.

A little assistance, please
For much of the 20th century, nursing homes were the institutions that took care of those unable to take care of themselves or be cared for by relatives or friends. Medicaid for low-income people fueled the growth of facilities with large medical staffs providing 24-hour care to residents in private or semi-private rooms. In many rural communities today, the local nursing home is the biggest and most stable employer in the area. (A 2013 economic analysis found that in Wisconsin, nursing homes employed more than 52,000 workers—more full-time equivalent jobs than in each of the paper, printing and lodging industries in the state.)
The ground started to shift under the long-term care industry in the 1980s, with growing interest in alternatives to nursing homes that reduced health care expenditures and gave the elderly and disabled more flexibility and choice.
“The market responded to consumers’ interests, wants and needs,” said Patti Cullen, CEO of Care Providers of Minnesota, an organization representing nursing homes and senior housing providers in the state. “Assisted living kind of bubbled out of the fact that people wanted a care setting that looked more homelike, that allowed for transitions, where as their needs increase they can pay for more services. That model was not available in nursing homes; it is available in assisted living.”
National data are scant on trends in assisted living, but a 2012 report by AARP, the association for people aged 50 and over, found that the number of assisted living and other community-based residential units increased 17 percent from 2007 to 2010, to 1.2 million. Meanwhile, nursing home use has declined; according to data from the U.S. Department of Health and Human Services, the number of occupied nursing home beds fell about 5 percent from 2003 to 2012.
Among district states, these trends are evident in Minnesota and Wisconsin, which have the most comprehensive data on changes in the number and capacity of long-term care facilities over the past two decades (see Charts 1 and 2).

In Minnesota, the number of housing-with-services providers—a category of senior housing that includes assisted living—has more than doubled since 2005, according to the state Department of Health. Meanwhile, the number of nursing homes has continued a decline that began in the late 1990s. In Wisconsin, state figures show that the capacity of assisted living facilities increased 48 percent between 2004 and 2014, while that of nursing homes fell 17 percent.
In a recent analysis co-sponsored by AARP, Minnesota and Wisconsin ranked first and second, respectively, among U.S. states in the number of assisted living and residential care units per 1,000 people aged 65 and over. Minnesota had over 91,000 units, a 70 percent increase since 2010.
Data for other district states on long-term care trends are incomplete, but nonetheless show growth in assisted living. In Montana, according to the state Department of Public Health and Human Services and AARP figures, the number of assisted living units has risen 30 percent over the past eight years, to over 5,600.
In North and South Dakota, assisted living has grown without significant reductions in nursing home capacity. In North Dakota, for example, the number of licensed assisted living units has risen by 48 percent to about 2,600 since 2006, but nursing home beds have fallen only slightly.
Government policy has facilitated the rise of assisted living, home care and other “consumer-centered” care models. Alarmed by the high costs of nursing home care, many states restricted the expansion of nursing homes. Minnesota enacted a statewide moratorium on the construction of new nursing homes and the licensing of additional nursing home beds in 1981. South Dakota has banned new nursing homes and beds since 1988, and North Dakota imposed its own moratorium on additional nursing home capacity in 1995.
Nursing homes in some parts of the district have shifted their focus to serve the very old or the sick—people who are bedridden after surgery or suffering from end-stage dementia, for example. In Minnesota, annual nursing home admissions have risen by about a third over the past decade, despite a drop in the number of licensed beds. Beds are turning over faster to accommodate convalescents admitted for short-term care after hospital stays.
State governments have also contributed to the growth of assisted living by developing Home and Community-Based Services (HCBS) programs to make community-based, long-term care accessible to the poor. In Minnesota, the Elderly Waiver program covers assisted living for people aged 65 and over who are eligible for Medicaid. Similarly, Wisconsin’s Family Care program provides support for Medicaid beneficiaries in a variety of long-term care settings.

A place for mom, with extras
Comparing assisted living development among states can be tricky because there is no single definition of assisted living. Unlike nursing homes, which are regulated by both the federal and state governments, assisted living is entirely state regulated. Rules in each state describe the scope of assisted living and set standards for accommodation and services offered to residents.
Many of these state rules determine how ill or infirm residents can become before they must be discharged to a nursing home or hospice. In Minnesota and Wisconsin, assisted living staff can help residents get in and out of bed and use the toilet, and provide other services almost on a par with nursing homes. This broad scope is one reason these states have seen so much growth in assisted living; providers can maximize revenues by providing more advanced services to residents as they age and their health declines.
Other states set the bar higher for residents’ capabilities (although in South Dakota recent legislation gives assisted living providers more latitude in caring for residents who need help with daily activities).
Assisted living providers—many of which are nonprofits such as churches and social service organizations—offer a range of options geared to their customers’ income level, tastes and state of health. “What I tell people about assisted living is that when you’ve seen one assisted living facility in Minnesota, you’ve seen one, because they’re all different,” said Cullen, of Care Providers of Minnesota.
As a rule, assisted living providers charge a monthly fee for room and board, which includes basic services such as laundry, housekeeping and one or two prepared meals each day. Additional services such as medication management, transportation to appointments and assistance with dressing and hygiene can add hundreds of dollars a month to the prices.
Housing styles range from elegant apartment complexes with lots of amenities to modest apartments or single rooms with access to communal dining and recreational areas. Upscale developments are more likely to be found in metro areas with higher average incomes. Folkestone, a year-old development on Lake Minnetonka in suburban Minneapolis owned by Presbyterian Homes & Services, features tastefully decorated apartments starting at $3,100 a month, ranging up to $4,200 a month for a two-bedroom apartment. Amenities geared to an affluent clientele include lap and therapy pools, a bistro, a movie theater and a beauty salon.

At the lower end of the price scale are small facilities, often extensions of nursing homes or converted private homes, in low-cost rural areas; in New Salem, Elm Crest charges about $1,450 a month for a one-bedroom apartment, a daily lunch and other basic services such as housekeeping, cable TV and garbage pickup.
Where state regulations allow, many assisted living facilities—sometimes separate units within large senior living campuses—specialize in caring for people with Alzheimer’s disease and other forms of dementia. This is the most expensive type of assisted living, comparable to or even exceeding the cost of nursing homes because of the intensity of around-the-clock care.
Prairie Senior Cottages operates six assisted living facilities in Minnesota for people with memory loss. Groups of no more than 10 people live in residential units with traditional floor plans and furnishings, sharing a kitchen and other communal areas to encourage social interaction. “Our niche is our small size and our true homelike feel,” said Chief Operating Officer Dustin Lee. The firm is planning to open a new location in Owatonna, Minn., this fall.
Assisted living isn’t just for the elderly; younger people with physical and mental disabilities are also gravitating toward this type of long-term care. In Wisconsin, adult family homes—small facilities licensed to house up to four residents—care for people of all ages with developmental disabilities and other debilitating conditions such as multiple sclerosis, traumatic brain injury, mental illness and drug addiction. The number of adult family homes in the state has doubled over the past decade.
A lower-cost model
On the continuum of long-term care costs, assisted living is a relative bargain; on average, assisted living residents pay considerably less for their accommodations and care than people in nursing homes.
A 2015 national survey sponsored by Genworth, a long-term care insurance firm, found that the U.S. median annual rate for assisted living in 2015 was slightly more than half the cost of nursing home care (see Chart 3). The cost differential between assisted living and nursing homes was even greater for some district states such as North Dakota and Wisconsin.
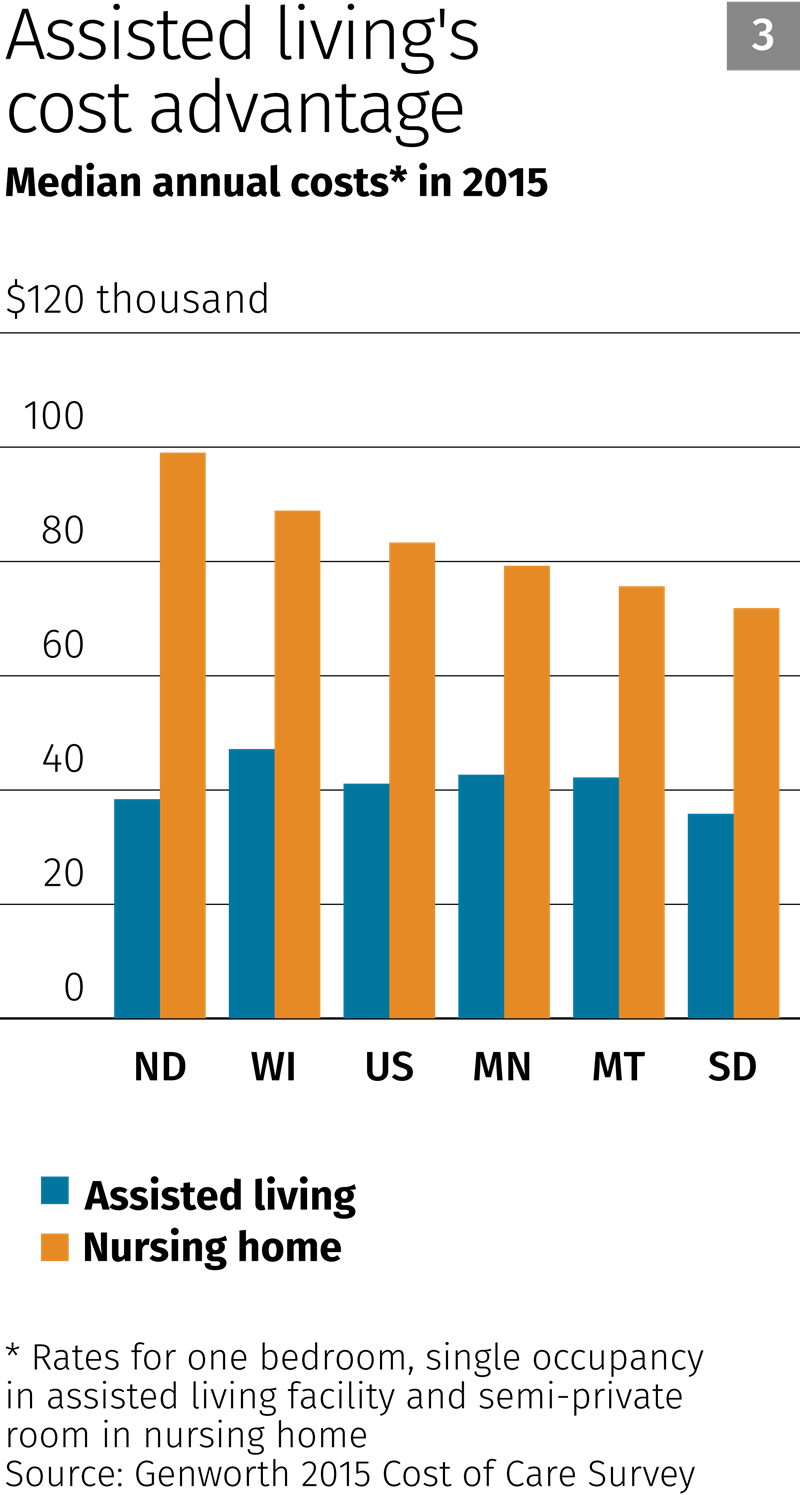
This cost gulf is to be expected, given the differences between the two models. In general, assisted living residents are younger and healthier and require less medical attention than people in nursing homes. This cuts labor expense, the biggest cost driver in long-term care; fewer nurses, nursing assistants and other staff are needed to care for residents of assisted living facilities.
Chris Krebsbach, vice president of operations for Tealwood Care Centers, a long-term care provider based in the Twin Cities, estimates that staffing levels at the firm’s 27 assisted living facilities in Minnesota and South Dakota are about 20 percent lower than those at its nursing homes.
At Elm Crest, one nursing assistant provides care to apartment residents, with Vogel (she’s trained as a nursing assistant) pitching in as needed. Other workers, such as cooks and housekeepers, are shared with the nursing home.
For the most part, assisted living is funded privately, out of residents’ pockets or through long-term care insurance. This is in sharp contrast to nursing homes, in which Medicaid and Medicare cover over half the total cost of resident care in most states. In North Dakota, 94 percent of assisted living revenue comes from private sources, according to the North Dakota Long-Term Care Association (about 20 percent of that is paid by insurers). However, anecdotal evidence suggests that districtwide, public funds make up a larger share of assisted living coverage in rural areas with lower median incomes.
Although only a small share of assisted living residents depends on public funding, the lower per capita care cost of assisted living provides relief for taxpayers footing the bill for long-term care by keeping low-income people who don’t require 24-hour care out of nursing homes.
But limited Medicaid funding restricts access to assisted living for the poor. As in nursing homes, compensation for the care of low-income residents often falls short of costs. A recent survey of Minnesota assisted living providers sponsored by Care Providers and LeadingAge of Minnesota found that on average, Elderly Waiver payments covered only 70 percent of the cost of services for residents’ assessed needs.
Some assisted living providers have no choice but to turn away HCBS-sponsored Medicaid recipients. In the past year, Prairie Senior Cottages has stopped accepting people on Elderly Waiver at some of its locations, limiting the program to current residents who have exhausted their private funds.
In South Dakota, which has comparatively low Medicaid reimbursement rates, assisted living providers accept few residents on HCBS, said Mark Deak, executive director of the South Dakota Health Care Association. “To be frank, it’s very difficult for assisted living facilities to even operate unless there is a fairly high ratio of private pay folks.”
This year, lawmakers in some district states increased Medicaid funding for assisted living, nursing homes and other types of long-term care. In Minnesota, legislation that created a new reimbursement system based on actual care costs included a one-time 5 percent budget increase for Medicaid waiver programs, making up for cuts in past years. The South Dakota Legislature granted a 3 percent funding increase for nursing homes and assisted living facilities.

Competing for caregivers
Nursing homes have long grappled with workforce problems because of low Medicaid reimbursement, which reduces revenues and wage levels, and the sometimes onerous nature of tending to the ill or the very old. Hiring and retention problems generally aren’t as dire in assisted living because staffing requirements are lighter, and higher levels of private funding let providers offer more generous wages. In addition, many workers find assisted living jobs more appealing than those in nursing homes.
But it’s still a tough labor market for assisted living facilities competing with hospitals and clinics for nurses, nursing assistants, housekeepers and other workers. Sources said other health care employers pay higher wages and often offer better working conditions and prospects for advancement.
Recovery from the Great Recession has worsened matters, said Kvenvold of LeadingAge. “We are countercyclical in terms of our workforce trends. When the economy is doing poorly, we find it easier to recruit and retain qualified employees. When the economy improves and there are options for better paying jobs with better benefits, unfortunately we don’t do as well.”
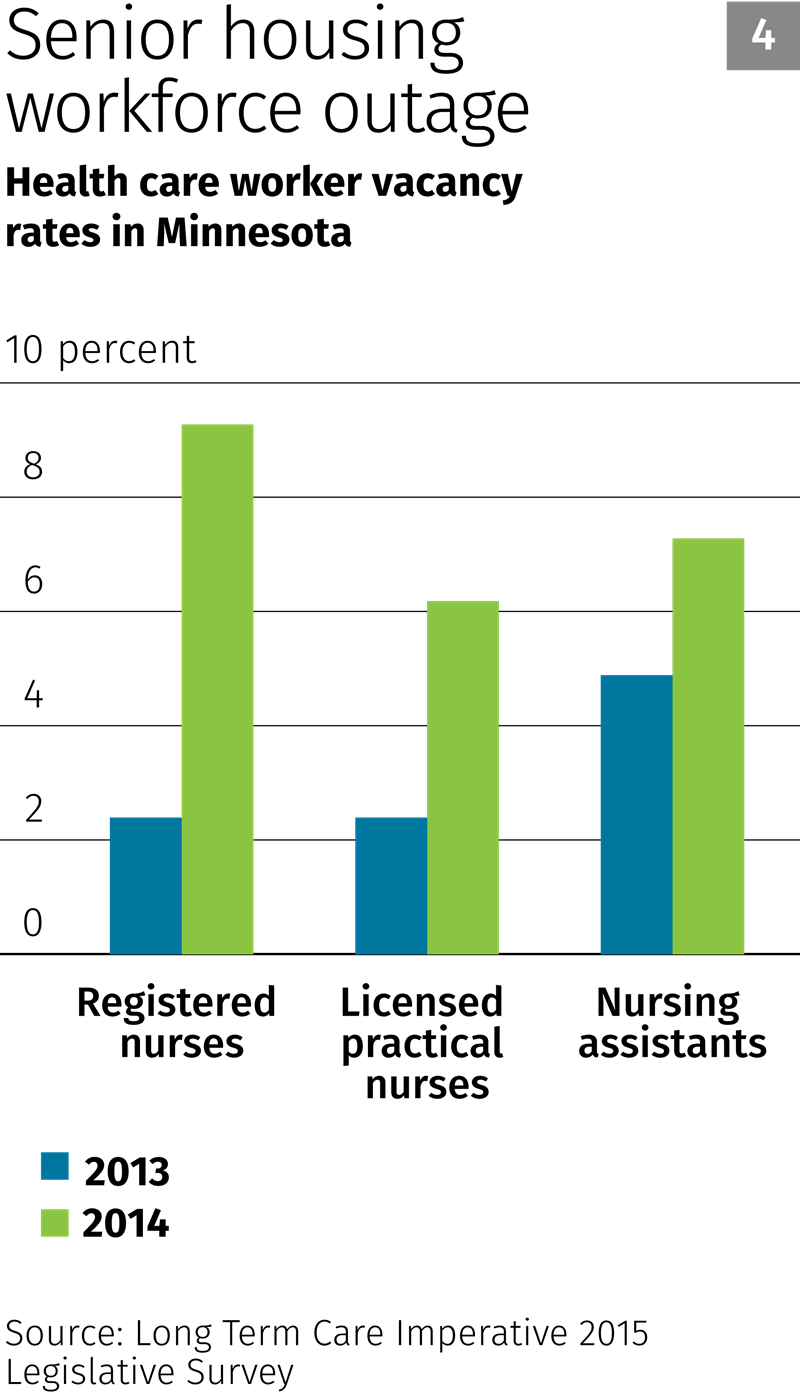
Job openings and turnover in assisted living facilities have increased in district states since the recession. A recent Minnesota survey sponsored by LeadingAge and Care Providers of Minnesota found that health care employee vacancy rates in senior housing (assisted living plus senior condominiums and apartments) increased from 2013 to 2014 (see Chart 4). Worker turnover also increased in the survey; annual turnover of registered nurses increased nine percentage points, to 25 percent.
At Tealwood, annual turnover was running about 35 percent at the firm’s two South Dakota locations near Sioux Falls and Aberdeen, and well over 50 percent at some facilities in Minnesota. “We really struggle in the rural areas because we have fewer people to draw from,” Krebsbach said. He added that Tealwood has opted not to expand in a few rural communities where a workforce analysis showed that health care workers were in short supply.
The firm’s recruiting and retention tactics include reimbursing the tuition of employees studying for nursing degrees and offering $500 to $1,500 sign-on and referral bonuses. Prairie Senior Cottages has taken a similar approach to hiring in a tight post-recession job market; this year, the firm started paying bonuses to workers who refer employees who stay at least three months, Lee said.
Despite its workforce challenges, assisted living is destined to remain a growth industry in the district by virtue of demographics. In Minnesota, the number of people over 65 is projected to increase by about 80 percent over the next 15 years, according to the State Demographer’s Office. The population of Minnesotans aged 85 and over is forecast to more than double by 2040. A similar age wave is expected to roll through other district states. The U.S. Department of Health and Human Services estimates that at least 70 percent of these aging baby boomers and their parents ultimately will need some form of long-term care.
For millions of people planning the final chapter of their lives, or coping with disability, assisted living has become the preferred model of long-term care. They are voting with their feet and their pocketbooks to remain independent for as long as possible, with a little help from others.
But the popularity of assisted living doesn’t mean that nursing homes will become extinct. Even with all the services that assisted living offers, skilled, around-the-clock nursing care is still necessary for those too frail and sick to lead a semi-independent lifestyle. “Assisted living is much less expensive than a nursing home,” said Jim Murphy, executive director of the Wisconsin Assisted Living Association. “But I don’t believe nursing homes should go away. There’s a need for that level of care, and there always will be. ... We can’t care for somebody that we can’t care for.”


